How to describe x-rays. Clinical diagnostics and radiography in veterinary medicine
X-ray for pneumonia. The photo shows an x-ray, which can be described as follows: The volumes of the lower lobes of both lungs are reduced. Their transparency is reduced due to the presence of compaction in the parenchyma, the decay cavity lung tissue on the right and pleural paracostal overlays on the left. Signs of the presence of free gas supraphrenic. Roots with a not very clear structure, compacted, the right one is widened in the tail. Costophrenic sinuses on the right are free, on the left they do not open. The shadow of the heart without features. Conclusion: Right-sided lower lobe destructive pneumonia, left-sided lower lobe pneumonia complicated by hydropneumothorax. 2
X-ray after surgical intervention with description The photo shows an x-ray, its description: The transparency of the lung tissue of the left lung is reduced due to the compaction of the parenchyma C-9, C-10 and pleural paracostal overlays. Linear tissue soup of segmental atelectasis in C-2 projection. A root with a not very clear structure. The anterior costodiaphragmatic sinuses do not fully open. On the right - the horizontal level of the epiphrenic, in the 4th intercostal space. The root is structural. The costophrenic sinuses do not open externally. The shadow of the heart is enlarged, the aorta is thickened, with calcium in the wall, the waist is smoothed. Recommended: ultrasound of the pleural cavity on the right. 3
X-ray picture for pleurisy with description The photo shows an x-ray picture. Description: The transparency of the lower lobe of the left lung is reduced due to the presence of encystation in the pleural cavity, along the posterior chest wall, at the level of the angle of the scapula. The pulmonary pattern is enriched due to bronchial and perivascular seals, thickened in the lower sections on the left. Roots with not very clear structure, compacted, with calcifications. Costodiaphragmatic sinuses are free on the right, do not open on the left (liquid). The shadow of the heart is somewhat dilated to the left, the aorta is thickened, with calcium in the wall. Conclusion: Pleurisy on the left. four

X-ray picture with encysted pleurisy with description The photo shows an x-ray picture with a picture of tuberculosis. Description of the image itself: The transparency of the lung tissue C9-10 on the right side is reduced due to the compaction of the parenchyma. The pulmonary pattern is enriched due to peribronchial and perivascular compaction, thickened in the lower sections on the right. Roots with a not very clear structure, displaced downwards, with calcifications. Costodiaphragmatic sinuses are free. The shadow of the heart without features, the aorta is sealed, with calcium in the wall. 6
RADIOGRAPH OF THE ORGANS OF THE CHEST CAVITY OF A PATIENT WITH PULMONARY EMPHYSEMA AND CHRONIC PULMONARY HEART cor pulmonale(direct projection): the heart is relatively small, the arc of the pulmonary cone (indicated by the arrow) bulges, the roots are expanded due to large branches pulmonary arteries, peripheral vascular pattern of the lungs is depleted 11
Gangrene of the lungs Gangrene is one of the most complex purulent diseases of the lungs. This disease is the death of rotten lung tissue due to the penetration and development of an infection in it, causing the process of suppuration. This process is accompanied by severe intoxication of the entire human body. The disease is accompanied by profuse discharge of putrefactive sputum with blood clots and pieces of dead tissue of the diseased lung. 12
Cancer of the apex of the lung with Pancoast's syndrome Pancoast's tumor or tumor of the superior sulcus of the lung (this name is more often used in the English literature) cancer of the first (apical) segment of the lung with Pancoast's syndrome. A growing tumor can compress or sprout the brachiocephalic vein (lat. v. brachiocephalica), subclavian artery (lat. a. subclavicularis), phrenic nerve (lat. n. phrenicus), recurrent laryngeal nerve (lat. n. laryngeus recurrens), vagus nerve (lat. n. vagus); typically compression or germination of the stellate ganglion (lat. ganglium cervicotoracicum s. stellatum), which causes the symptoms of Horner's syndrome. fifteen
Percussion over a homogeneous airy thin-walled cavity also gives a long, low and loud sound, moreover, a musical tone due to additional overtones that are harmonious with the main percussion tone. Such a percussion sound is called tympanic, as it resembles the sound that occurs when a drum is struck (tympanum on). A tympanic sound normally occurs on percussion of the abdomen, since the abdominal cavity is filled with loops of intestine containing gas, and ^ skin on percussion in the lowest part of the anterior surface of the left half chest above the "air bubble" of the stomach (Traube's space). 19 Emphysema
Pheochromocytomas of the adrenal glands. Radiography: the formation in the adrenal gland deforms the upper pole of the kidney and is separated from it by a thin layer of fiber. 25 Radiography: a mass in the adrenal gland deforms the upper pole of the kidney and is separated from it by a thin layer of tissue.
Peripheral lung cancer On roentgenograms of the chest organs in direct, right lateral projections, tomograms of the right apex revealed a rounded formation adjacent to the side wall with a wide base. Dimensions 13 x 9 cm, with fairly clear, polycyclic contours; homogeneous. 26 straight right side right

A complete orthopedic examination is mandatory before X-rays (RS) are taken, as X-ray diagnosis does not always coincide with clinical diagnosis.
The general rules for performing RS are also applicable to the knee joint (KJ), these include the following:
It is necessary to perform RS in at least two orthogonal projections, observing the correct laying
Do not try to interpret poor quality photographs
If the patient is not calm or in pain, anesthesia is performed.
In doubtful cases, images of the contralateral joint may be useful - it is important to observe centering on the area of interest and framing to capture all adjacent structures.
The most common findings in MS of the knee are secondary degenerative changes such as osteophytes, subchondral bone sclerosis. Osteophytes are located on the tops of the patella, sesame bones, above the femoral groove and along the border of the cartilage, in the intercondylar fossa and near the condyles of the tibia. A frequent finding is an increase in the volume of soft tissues, the accumulation of joint fluid (determined by the displacement of the shadow of the infrapatellar fat body), calcifications in the projection of the anterior cruciate ligament (ACL). To assess the intercondylar fossa, RS is performed in a special laying, so that the rays pass perpendicular to the femoral condyles.
Less common are signs of dissecting osteochondritis (visible in direct projection), avulsion of the tendon of the long extensor of the fingers, separation of the attachment site of the anterior patellar ligament (visible in lateral projection in a state of hyperflexion of the knee joint).
When evaluating the valgus deformity of the thigh, the correct laying in the direct projection is controlled by the median position of the kneecaps. The normal external angle between the axis of the thigh and the line drawn through both condyles is 90 - 95°. To rule out an erroneous diagnosis of valgus deformity of the lower leg, suspected in images with pronation of the extremities, the RL of the lower leg is performed in a direct projection, placing the foot in the sagittal plane. The normal angle between the axis of the lower leg and the straight line drawn through the articular surfaces of the lower leg is about 90°.
In case of dislocation of the patella, pictures are taken in a direct projection, and the normal location of the patella in the projection of the intercondylar groove does not exclude dislocation of 1-2 degrees. It is possible to assess the medial displacement of the tibial tuberosity by controlling the correctness of the direct projection in the position of the metatarsus. To assess the gutter and the usual position of the patella, a contour projection of the knee joint is performed.
X-ray is not an expert method for diagnosing ACL rupture, it only allows you to identify secondary changes. However, to perform corrective surgeries with osteotomy of the proximal tibia, it is necessary to perform radiography to determine the angle of inclination of the tibial plateau relative to its axis, which is normally 20-25°. The normal slope of the plateau does not exclude ACL rupture. Before performing TTO, the correction angle is calculated, i.e. the angle between the perpendicular to the plateau and the straight line passing along the patellar ligament.
The most common errors in the interpretation of MS are: interpretation of the fossa of attachment of the extensor digitorum longus or popliteal muscle as a pathological defect; false assessment of the angle of inclination of the tibial plateau due to rotation of the lower leg or incorrect centering of the beam, attempts to exclude diagnoses of ACL rupture or medial dislocation of the patella according to RS, taking growth zones for fracture lines.
In dogs with a partial anterior cruciate ligament tear, it can be difficult to detect PCOS, so high-quality x-rays are needed to detect changes in the joint and, often, early signs degenerative joint disease Kotelnikov G.P., Kuropatkin Gn., Pivovarov M.V. Forms of post-traumatic instability of the knee joint // Orthopedics, Traumatology and Prosthetics. - 2011. - No. 9. - P. 5-9 ..
X-ray images of the knee joint must be made in principle in two planes - in the anterior-posterior projection and lateral. If the joint is fixed in a slightly flexed position, then the X-ray tube must be rotated for an anteroposterior image so that a true image of the joint space is obtained. At the same time, for comparison, x-rays of both knee joints are taken. degenerative disease in the opposite joint may have diagnostic value suggesting an increased likelihood of cranial cruciate ligament rupture compared with dogs that do not have such joint disorders.
animal diagnosis x-ray
Fig.1. Lateral radiographs of the knee
X-ray signs of ACL rupture are due to the displacement of the condyles of the tibia forward in relation to the femur.
Radiographs may also show areas of bone in young animals with lacerations, as well as cranial subluxation of the tibial eminence relative to the femoral condyles. In radiographic diagnosis, the assessment of the state of the intercondylar fossa is important. In dogs with chronic knee instability associated with ACL rupture, the intercondylar fossa gradually narrows due to the development of osteophytes on its inner surface. Congenital narrowness or deformity of the intercondylar fossa can also cause rupture of the ACL itself or the grafts used to reconstruct it. Despite this fact, the effect of stenosis of the intercondylar fossa on the outcome of intra-articular ACL reconstruction in dogs is unknown. On conventional radiographs of the knee joint in craniocaudal or caudocranial projections, the fossa is indistinct. However, it is clearly visible when laying the dog in the dorsal recumbent position, with the hip and knee joint bent, directing the radiation axis perpendicular to the femoral condyles. Radiography is carried out in two projections - direct and lateral Lindenbraten LD, Naumov LB// Medical radiology. -M.: Medicine, 1984. S. 113 ..
The resulting images were evaluated according to the following indicators:
Change in the axis of the femur to the tibia
Increase or decrease in the joint space.
Displacement of articular surfaces relative to each other and the axis of the joint.
The presence of chondromatous growths on the articular surfaces and the patella.
The presence of damage to the articular surfaces in the form of exfoliation of hyaline cartilage ("articular mouse"), changes in the configuration of the condyles and the patella.
Displacement of the sesamoid bone of the popliteal muscle distally relative to the horizontal level of the tibial plateau.
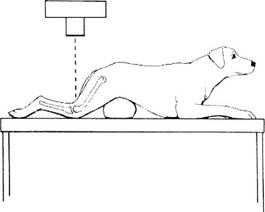
Rice. 2. Schematic representation of the correct position of the animal to obtain a radiograph of the intercondylar fossa. The animal was fixed in the thoracic lying position, a pillow was used to raise the abdomen.


Fig.3. a - radiograph of the knee joint of a dog with ACL rupture; b - radiograph of the dog's knee joint after triple tibial osteotomy

Fig.4. Rupture of the anterior cruciate ligament (displacement of the center of the femoral condyles relative to the center of the tibial plateau). Reducing the angle between the axis of the tibial shaft and the plateau.
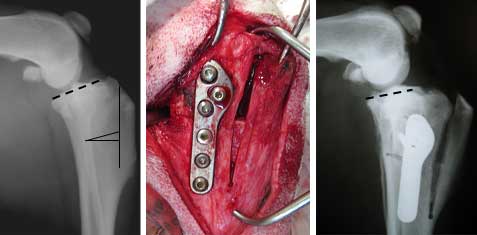
Fig.5. Stabilization of the knee joint according to the TOT method
Stabilization of the knee joint occurs due to an increase in the angle between the axis of the diaphysis and the plateau of the tibia, as well as due to the displacement of the tuberosity of the tibia, which pulls the direct patellar ligament and collateral ligaments of the patella cranially, which also contributes to the stabilization of the knee joint.
Knee arthrography is necessary when conventional clinical and radiographic examination methods are not sufficient to recognize a knee lesion. The puncture is performed from the outside approximately at the level of the middle of the patella, slightly posterior to the articular surface of the patella. The injection site is anesthetized with 1% novocaine solution. Check the position of the needle with novocaine (as in arthrography of the hip joint). Joint fluid and novocaine solution are removed before injection of a contrast agent by pressing on the upper inversion and from below the joint. After possible emptying, 3-4 ml of cardiotrast solution (urotrast or triombrin) is injected into the joint cavity. Sometimes, with the introduction of a contrast agent, the upper inversion is squeezed with tours of an elastic bandage. Take the required number of x-rays, having prepared in advance the appropriate number of cassettes, since the shadow of the contrast agent almost completely disappears after 20 minutes. Produce the appropriate image depending on the conditions in a particular position 1) anteroposterior image with a slightly caudally directed tube, the knee joint is unbent; 2) lateral internal-external image. Errors in the execution technique occur when the contrast agent is unevenly distributed, most often because they forget to make several passive movements after injection. It is also possible that movements are not possible due to a blockage or limitation of mobility.
To date, the most accurate method for diagnosing damage to the ligamentous apparatus and menisci of the knee joint is magnetic resonance imaging (MRI).
In certain cases, arthroscopy may be used. This surgical procedure consists in introducing a special device with a microvideo camera into the joint cavity. It is indispensable in case of suspected ACL tear and meniscal injury Yagnikov S.A. Stabilization of the knee joint in dogs with torn anterior cruciate ligament. " Vet clinic". 2005.1, 26-29..
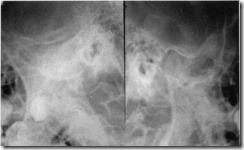
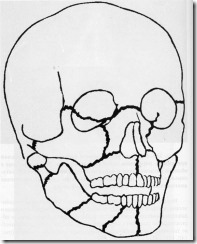
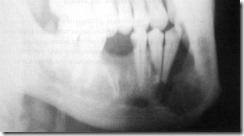
X-ray of the left side mandible. Cortical plate (1), teeth (2), large-loop spongy substance in the region of the body of the lower jaw (3).
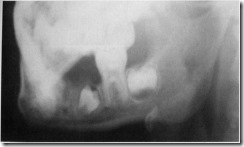
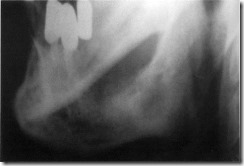
X-ray of the right half of the lower jaw of a 4-year-old child. Barely noticeable signs of mineralization of the rudiment of the permanent lower fifth tooth (indicated by an arrow).
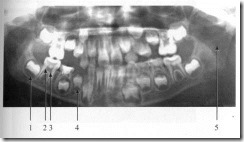
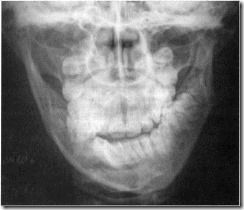
Orthopantomogram of a 7-year-old child. The follicle of the second permanent molar (1), the cavity of the tooth (2) and the root canal (3) of the permanent first molar, the unformed roots of the first permanent premolar and the remains of the follicle at its apex (4), the air column of the upper respiratory tract (5).

Mandibular canal (1) and mental foramen (2) on an orthopantomogram of an 8-year-old child.
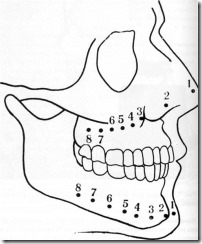
Projection on the face of the upper and lower teeth used in dental radiography
Dental radiography
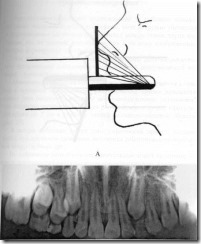
The relationship between the X-ray machine, the object and the film in the examination of teeth on upper jaw.
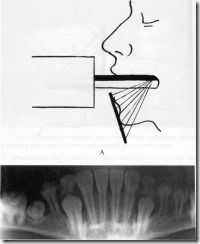
The relationship of the X-ray apparatus, the object and the film in the study of the anterior teeth in the lower jaw.
The relationship of the X-ray apparatus, the object and the film in the study of the lateral teeth in the lower jaw.
The relationship of the X-ray machine, object and film during a dental snapshot "bite".
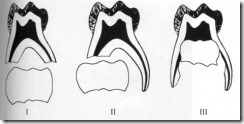
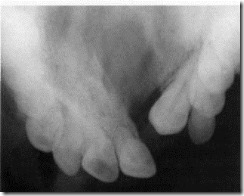
Three types of resorption of the roots of milk teeth: I - uniform reduction in the length of the roots, II - uneven and III - resorption of the bifurcation.

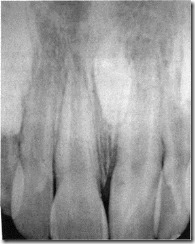
The position of the rudiments of permanent incisors on a detailed radiograph 6 summer child. Resorption of the roots of the upper central milk incisors according to the first type.

Destruction by the carious process of IV and V teeth on; antal radiograph of an 8-year-old child. Resorption of the roots of the fourth baby tooth according to the third type, the fifth - according to the first 
The relationship of the x-ray machine, object and film during panoramic radiography.
Scheme of the position of the X-ray tube in the patient's mouth during panoramic radiography of the upper dentition and its image in the image.
The position of the X-ray tube when held! panoramic radiography of the lower dentition and its image in the picture. Scheme of the position of the x-ray tube of the patient's oral cavity during a panoramic x-ray of the lower dentition and its image on the city.
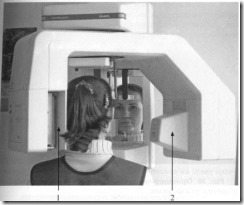
The position of the subject's head in relation to the film cassette (1) and X-ray tube (2) during orthopantomography.

Orthopantomogram of a 15-year-old child with an anomaly in the position of the upper frontal teeth pushed to the sides by an intramaxillary tumor - odontoma (indicated by an arrow).

Orthopantomogram of an 8-year-old child with normal development of the dentition.

Orthopantomogram of a 38-year-old patient with chronic generalized periodontitis, characterizing the degree of atrophy of the alveolar bone tissue. Retention and dystopia of the eighth teeth on the lower jaw on both sides and on the upper jaw on the right, partial secondary adentia.

Orthopantomogram of a 17-year-old patient with a mesial bite in combination with an open one, performed at the stage of orthodontic treatment.

Orthopantomogram of a 32-year-old patient in need of orthopedic treatment with secondary adentia in the region of the left half of the upper dentition.
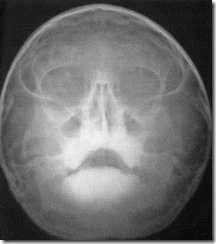
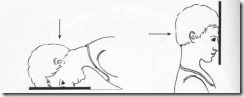
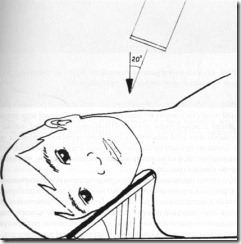
The relationship of the examined, x-ray I parat and film in x-rays of the upper jaw (nose-chin laying).

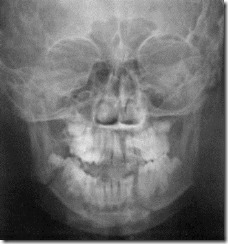
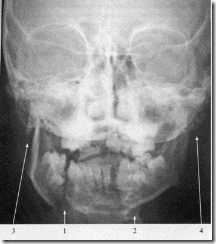
X-ray of the facial skeleton, taken in the naso-chin position to assess the condition of the upper jaw. A decrease in the airiness of the right maxillary sinus and cells of the ethmoid labyrinth, thickening of the turbinates, curvature of the nasal septum and its displacement to the left are determined.
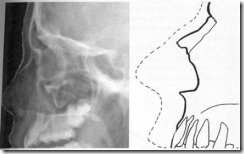
X-ray of the facial skeleton in profile and its schematic representation.
The relationship of the subject, X-ray apparatus and film in the X-ray of the upper jaw in the axial projection.
Axial radiograph of the facial skeleton.
The relationship of the subject, the X-ray apparatus and the film during the survey radiography of the lower jaw (naso-frontal styling).

X-ray of the facial skeleton of a 15-year-old patient performed in the naso-frontal position to assess the condition of the lower jaw.
The relationship of the subject, the X-ray apparatus and the film in the X-ray of the lower jaw.

The radiograph of the lower jaw was carried out in compliance with the basic methodological requirements.

Method of X-ray examination of the temporomandibular joint with a closed and open mouth.
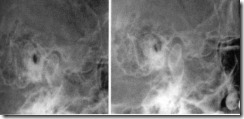
X-rays in the Schüller layout with a schematic representation of the temporomandibular joint with a closed (A) and an open mouth (B).

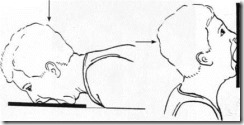
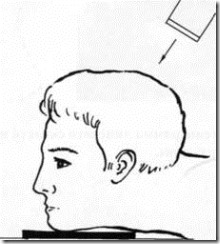
The method of performing a teleroentgenogram of the skull

Teleroentgenogram of a patient D. with underdevelopment of the lower jaw
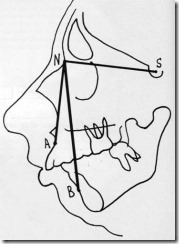
Unchanged on the teleroentgenogram of patient D. c, the mask of the SNA angle with a decrease in the SNB angle indicates a normal position in the skull of the upper jaw and distally) displacement of the mandibular arch.

Teleroentgenograms of a 16-year-old patient before (A) and after elimination of anterior protrusion of the lower jaw (B).

A radiograph with artificial contrasting, specifying the direction of the congenital fistula of the submandibular salivary gland on the right in patient N. There is a tight filling of the linear fistulous course of uneven width with a radiopaque substance.

X-ray of the lower jaw of a 15-year-old patient with a contrast agent injected into the tumor-like formation of the submental region, confirming the presence of a median cyst of the neck.


X-ray sialadenograms in frontal and lateral projections of an 11-year-old patient with chronic parenchymal parotitis (frontal and lateral projections). The intraglandular ducts are passable, there is a defect in filling the right parotid salivary gland with a contrast agent, in the final sections small cavity formations of various sizes and shapes are filled.
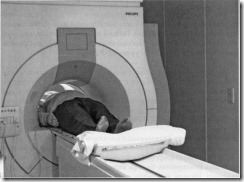
Apparatus for performing computed tomography.
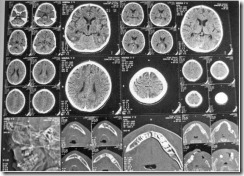
Computed tomography of the skull: axial sections at different depths with magnification, reconstruction in bone tissue mode during restoration of the lower jaw.
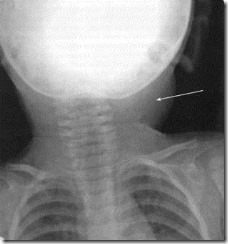
The shadow of a soft tissue tumor formation of a homogeneous structure in the region of the lateral surface of the neck on the left on the radiograph of patient A.
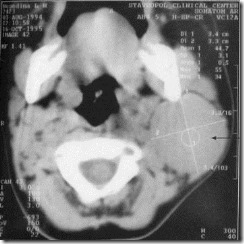
Computed tomogram of patient A. with a neck tumor. On the left, a homogeneous, solid formation measuring 3.5 cm in diameter, rounded in shape with a clear contour. According to the results of densitometry, its density in accordance with the Haunsfield scale is 44.7 units. N.
Computed tomography of an 11-year-old patient with fibrous osteodysplasia of the temporal bone on the left. The thickness of the temporal bone on the left is 2-3 times thicker than the opposite side.
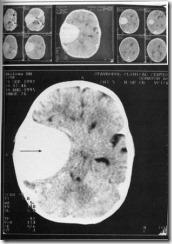
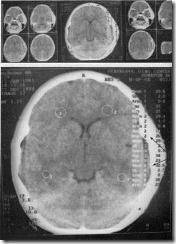
Computed tomography of a patient with a brain tumor. In the temporo-parietal region on the right, a parietal compaction of tissues of a homogeneous structure is determined, with a wide base adjacent to the bone tissue (indicated by an arrow). Taking into account serial sections, it is possible to assume the presence of meningioma.
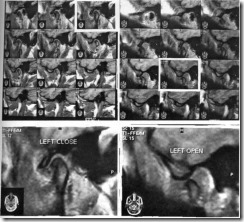
Magnetic resonance imaging of the left temporomandibular joint of a patient with chronic arthritis, with closed (A) and open mouth (B). In serial images, one section is highlighted with a white frame and presented in an enlarged image.
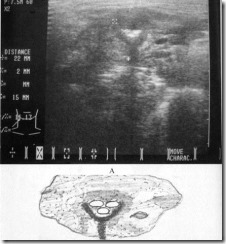
Ultrasound computed tomography of a patient with lymphadenitis of the submandibular region on the right (A) and a schematic representation of the identified object (B). Echopicture: at the level of the angle of the lower jaw on the right, the reaction of regional lymph nodes in the form of a group of hypoechoic rounded additional structures of uniform density, with clear, even contours.

Dental radiograph of the alveolar process of the upper jaw. Destruction by the carious process of the contact surfaces of the crowns of the upper first and second premolars.

Dental radiograph of the lateral fragment of the alveolar part of the lower jaw. Destruction of the crown of the lower first molar by a carious process and communication of the hard tissue lesion with the tooth cavity.
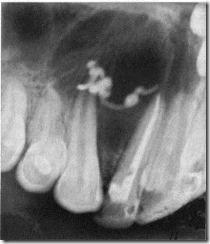
Dental radiograph of the alveolar process of the upper jaw. The expansion of the periodontal gap in the region of the upper first premolar and a slight enlightenment of the bone tissue around its apex, a crown defect due to a deep carious lesion, the tooth cavity and root canal are filled with filling material to the root apex.

Dental radiograph of the alveolar process of the upper jaw. A focus of bone tissue destruction with a clear contour in the region of the tops of the roots of the upper first premolar (1), at the roots of the sixth tooth, an air-filled lacuna of the maxillary sinus is visible (2).

Orthopantomogram of a 9-year-old patient with follicular cyst lower jaw on the left. Defect of bone tissue of the lower jaw on the left with a clear contour, limited by the zone of sclerosis. The rudiments of the permanent canine and premolars, located in the zone of destructive damage, are pushed to the lower edge of the jaw.
Dental radiograph of a patient with a radicular cyst of the upper jaw from the upper lateral incisor. The removal of a radiopaque filling material through the canal of the lateral incisor into the cavity of the periradicular cyst is an erroneous attempt to treat a large cyst in a conservative way.

Plain radiograph of the facial skeleton and dental image of the frontal area of the alveolar process of the upper jaw of an 11-year-old patient with a left-sided cleft upper lip and the sky. Asymmetry of the pear-shaped openings and curvature of the nasal septum, a change in the shape of the upper dentition and an anomaly in the position of the teeth on both sides of the defect of the alveolar process.


Plain radiograph of the facial skeleton and dental image of the frontal area of the alveolar process of the upper jaw of a 12-year-old patient with bilateral cleft lip and palate. Anomaly in the shape of the upper dentition, bilateral defect of the alveolar process and hard palate, anomaly in the shape and position of the upper anterior teeth.

Dental radiograph of the lateral section of the upper dentition of a 15-year-old patient with retention and dystopia of the permanent upper canine. Its place in the dentition is occupied by the milk canine destroyed by the carious process, at the top of the root of which there is a focus of bone tissue destruction with an even, clear contour.
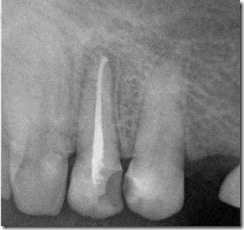
Dental radiograph of the frontal section of the upper dentition of a 13-year-old patient with an anomaly in the position of the upper central incisors due to a supernumerary impacted tooth. The roots of the upper central incisors are separated to the sides, between them there is an oval-shaped radiopaque formation with an even contour, corresponding in density to the crown part of the tooth.

Orthopantomogram of a 14-year-old patient. A supernumerary tooth in the frontal area of the upper dentition (1), which caused confusion and delay in eruption of the permanent upper left central incisor (2).

Orthopantomogram of a 15-year-old patient with an odontoma of the upper jaw on the right, which caused retention and dystopia of the upper right canine. Odontoma in the form of a dense heterogeneous structure formations between the roots of the upper central and lateral teeth on the right (1), above it is located in a semi-horizontal position the upper right canine with a formed root (2).

Orthopantomogram of an 11-year-old patient. Anomaly in the position of the upper permanent incisors, retention and dystopia of the upper canines. Primary edentulous upper permanent lateral incisors and first premolars. Primary edentulous permanent lower first premolars and second molars.
![]()
106. Orthopantomogram of an 18-year-old patient with an open bite. Violation of the closure of the dentition within the incisors, canines and first premolars.

Orthopantomogram of a 16-year-old patient with a violation of the ratio of the dentition according to the III class of the Angle classification in combination with an open bite. The protrusion of the lower dentition anteriorly along with the sixth teeth and the separation of the bite throughout the dentition. Articulation is preserved only on the seventh teeth.

Orthopantomogram of a 16-year-old patient G. with crowded position of the upper teeth and a mesial ratio of the dentition in combination with an open bite.
Plain radiograph of the facial skeleton of a 17-year-old adolescent with crossbite. Asymmetric shape of the mandibular arch as a result of shortening of the body and the branch of the mandible on the left. Violation of the shape and relationship of the dentition.

Teleroentgenogram of the facial skeleton of a 16-year-old patient with an anomaly in the position of the upper teeth, a shortening of the longitudinal size of the upper dentition and an open bite.

X-ray of the lower jaw of an 8-year-old child with odontogenic periostitis. Destruction by carious process of the crown of the first lower molar. The focus of bone tissue destruction around its anterior root continues to the lower edge of the jaw body, where the shadow of the periosteum exfoliated from the bone is determined in the form of a semicircular formation adjacent to the compact layer with a wide base.

X-ray of a 13-year-old patient with acute osteomyelitis of the lower jaw. Foci of bone tissue destruction at the roots of the first molar destroyed by the carious process (1), extending to the spongy substance (2) and the compact layer (3) of the body of the lower jaw.

X-ray of the lower jaw of a 19-year-old patient with chronic destructive osteomyelitis of the lower jaw. Multiple foci of destruction of the bone tissue of the body of the lower jaw (1). As a result of destruction, the cortical layer loses its shape (2). In the destroyed areas of the spongy tissue, fragments of increased density of different sizes are determined - sequesters (3).

X-ray of the lower jaw of a 5-year-old patient N. with chronic osteomyelitis at the stage of recovery. In the area of the body of the lower jaw around the rudiments permanent teeth the formation of young bone tissue is noted.

Radiographs of the temporomandibular joint of a patient with acute arthritis with closed (A) and open mouth (B). Uneven narrowing of the anterior-upper parts of the joint space with a closed mouth (indicated by an arrow).

Orthopantomogram of a patient with deforming arthrosis of the temporomandibular joint on the right. Hypoplasia of the bone structure of the branch and body of the lower jaw on the right - a symptom of "heel" (1), shortening, hypoplasia and change in the shape of the articular head (2).
Radiographs of the temporomandibular joints on the right (A) and left (B) of a patient with right-sided ankylosis. Absence of an X-ray joint space in the area of the right temporomandibular joint and compaction in this area of the bone tissue due to osteosclerosis.
|
|

Radiographs of the facial skeleton of a patient with salivary stone disease of the left submandibular salivary gland. A rounded radiopaque shadow of a foreign body in the submandibular region on the left is indicated by an arrow.
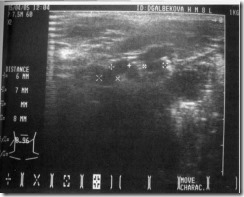
Ultrasound of a patient with salivary stone disease of the submandibular salivary gland and a schematic representation of the identified stones. Echo picture: the submandibular salivary gland is enlarged in size with a wavy and uneven contour, signs of a diffuse decrease in the echo density of the parenchyma of the gland and the presence of three rounded additional structures (calculi) in the central section.

Plain radiograph of the facial skeleton of a patient K. with a gunshot wound (laying in the naso-frontal position). Radiopaque foreign body in the projection of the right maxillary sinus of a homogeneous structure, with a clear contour, denser than the tooth tissue.

Plain radiograph of the facial skeleton of a patient K. with a gunshot wound (lateral projection). A rectangular-shaped, radiopaque foreign body with a metal density is located behind the posterior wall of the maxillary sinus.
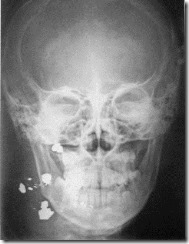
Plain radiograph of the facial skeleton of patient A. with a wound maxillofacial region from a hunting rifle (laying in the nose-frontal position). Radiopaque injuring objects of various sizes and shapes (buckshot) in the area of soft tissues of the right half of the face have metal density and clear contours.

Plain radiograph of the facial skeleton of patient A. with a wound in the maxillofacial area from a hunting rifle (lateral projection). Along with small foreign bodies in the form of point formations in the lower third of the face, six larger radiopaque foreign bodies are determined.
Probable localization of fractures of the jaw bones in trauma.
Plain radiograph of the facial skeleton of patient Yu. with a bilateral fracture of the lower jaw (laying in the naso-frontal position). Violation of the integrity of the bone tissue of the lower jaw in the area of the angle on the right and the mental area on the left, the formation of a step along the fracture line in the contour of the lower edge of the jaw due to the downward displacement of the middle jaw fragment.
Plain radiograph of the facial skeleton of a patient K. with a multiple fracture of the lower jaw (laying in the naso-frontal position). Violation of the integrity of the bone tissue along the line of a double fracture of the body of the lower jaw (1 and 2) and violation of the contour of the distal parts of the lower jaw as a result of a bilateral fracture of the condylar processes (3, 4).

Plain radiograph of the facial skeleton of patient Y. with a fracture in the region of the angle of the lower jaw on the right after reposition and fixation using double-jaw splints and elastic traction according to the Tigirstedt principle. Unsatisfactory result of treatment: pronounced displacement of the distal fragment (branches) deprived of teeth after a conservative method of reposition and fixation of jaw fragments.

Plain radiographs of the facial skeleton of patient S. with a comminuted fracture of the body of the lower jaw on the right after surgical treatment. Reposition and fixation of bone fragments of the body of the lower jaw with a wire loop.

Roentgenogram of the lower jaw of a patient Ya. with a fracture of the body of the lower jaw after surgical treatment with the use of an extraosseous metal staple and wire sutures: complete convergence of the bone fragments was ensured.

X-ray of the lower jaw of a patient Zh. with a fracture of the lower jaw branch after surgical reposition and fixation of fragments with an intraosseous pin.

Plain radiograph of the facial skeleton of patient D. with a fracture of the lower jaw on the right. The result of surgical treatment using an extraoral compression-distraction apparatus and dental wire splints with elastic traction.

Plain radiograph of the facial skeleton of a patient Ch. with a defect in the chin and the body of the lower jaw after a gunshot wound. Fragments of the lower jaw were fixed using the Rudko apparatus.

X-ray of the lower jaw of a 17-year-old patient with hyperparathyroid osteodystrophy (Recklinghausen's disease). Rounded area of destruction in the area of the body of the lower jaw with a blurred contour without a clear demarcation from healthy bone tissue.

Plain radiograph of the facial skeleton of a patient with fibrous dysplasia of the lower jaw on the right. Uniform increase in bone density and contour of the right half of the lower jaw without a clear delimitation from the healthy parts of the jawbone on the left.

Orthopantomogram of a patient with ameloblastoma in the region of the angle of the lower jaw on the left. The center of destruction of bone tissue is rounded in the region of the angle of the lower jaw on the left, surrounded by a light rim of sclerotic bone tissue. There is a displacement to the rear wall of the cavity formation of the rudiment of the left eighth tooth. The roots of the lower seventh tooth are pushed forward until they come into contact with the roots of the neighboring lower sixth tooth.

X-ray of the right half of the lower jaw of a patient with ameloblastoma. An extensive focus of bone tissue destruction from the canine to the middle of the branch with a clear contour is surrounded by a dense rim of sclerotic bone tissue. Severe deformation of the contour of the lower jaw, which has the character of swelling in the area of the body, angle and branch.

Plain radiograph of the facial skeleton of patient X., 11 years old, with a solid complex compound odontoma. X-ray contrast formation in the area of the angle and branch of the lower jaw on the right, delimited from healthy areas of the jawbone by a sclerotic strip.

X-ray of the lower jaw of a patient X. 11 years old with an odontoma of the lower jaw. In the lower pole of the radiopaque formation, located in the area of the angle and branch, the crown of the permanent molar with unformed ones is determined.
X-ray of the lower jaw of a patient with a peripheral form of osteoblastoclastoma. Marginal defect of the alveolar process with a clear lower contour as a result of resorption of the bone tissue above the rudiment of the permanent fifth tooth.
X-ray of the lower jaw of a patient with a central form of osteoblastoclastoma. The destruction of the bone tissue of the body of the lower jaw in the area of the fourth and third teeth has the character of a multi-chamber formation with a clear contour and a line of osteosclerosis that limits individual cavities.

Plain radiograph of the facial skeleton of patient E. with central osteoblastoclastoma of the chin and the left half of the lower jaw. The shape of the lower jaw is drastically changed by the neoplasm, which has the character of a multi-chamber formation outlined by a zone of sclerosis of the bone tissue.

Lateral radiograph of the facial skeleton of patient E. with central osteoblastoclastoma of the chin and the left half of the lower jaw. The neoplasm, outlined by the zone of sclerosis of the bone tissue, has the character of a multi-chamber formation that changes the shape of the lower jaw.
![]()
Plain radiograph of the facial skeleton of a 65-year-old patient N. with an osteolytic form of osteogenic sarcoma of the lower jaw branch on the left. Destructive lesion of the condylar process of the lower jaw on the left with indistinct blurred borders.
X-ray of the lower jaw of a patient with fibrosarcoma of the body of the lower jaw. Foci of destructive damage to the body of the lower jaw from the mental foramen to the corner with blurred fuzzy boundaries.

Dental radiograph of the frontal section of the alveolar process of the upper jaw of a patient after treatment of the central and lateral incisors for chronic periodontitis.
Protocol:
On the dental radiograph of the alveolar process of the upper jaw, a defect of 1/3 of the crown part of the central incisor associated with the tooth cavity, a uniform expansion of the periodontal fissure along the entire length of the roots of the central and lateral incisors is determined. The root canals of the central and lateral incisors are wide, filled with filling material with partial removal of it beyond the top. At the tops of the roots of these teeth, there is a formed focus of bone tissue destruction with an indistinct contour.
Examples of radiograph descriptions
![]()
Orthopantomogram of a 64-year-old patient with severe chronic generalized periodontitis.
Protocol:
On the orthopantomogram, the second lower molars are inclined towards the missing lower first molars, the roots of the premolars are bare by 1/2, the incisors - by 2/3. Deep bone pockets and signs of osteosclerosis are determined around the roots. The alveolar margin of the lower jaw is smoothed and does not have natural serrations in the interdental spaces. Atrophy of the alveolar process of both jaw bones is determined, osteoporosis is predominantly of the horizontal type mixed genesis(involutive and odontogenic).
Examples of radiograph descriptions

X-ray of the lower jaw of a patient with odontogenic osteomyelitis after the removal of the causative tooth.
Protocol:
On the radiograph of the lower jaw, the hole of the removed sixth tooth with blurry fuzzy walls is determined. There is uneven destruction of the bone tissue of the jaw body from the canine to the second molar. The lesion is represented by areas of low density without clear contours with islets of osteonecrosis (single small sequesters) alternating with foci of increased density (osteosclerosis). The compact layer in the region of the lower edge of the jaw is destroyed in a limited area; soft tissues compacted.
Conclusion: the indicated X-ray picture corresponds to the transition of acute odontogenic osteomyelitis of the lower jaw to the chronic stage.
Examples of radiograph descriptions

Plain radiograph of the facial skeleton of a patient with ameloblastoma of the body, angle and branch of the lower jaw on the right.
Protocol:
On the survey radiograph of the facial skeleton in the naso-frontal projection in the area of the body, angle and part of the jaw branch on the right, an oval-shaped focus of bone tissue destruction with signs of swelling of the jawbone and thinning of its cortical layer is determined. Bone tissue defect of homogeneous structure with a clear band of osteosclerosis along the entire perimeter.
Conclusion: X-ray picture of a benign soft tissue tumor, corresponding in all respects to ameloblastoma.
Novice radiologists often face the problem of lack of methodological literature. Books by old authors are not reprinted, modern ones are largely devoted to high technologies and rarely to pressing issues of daily, routine work.
This material was prepared at the request of novice colleagues and contains schemes for analyzing radiographs and recording radiographic studies. It opens a new section of the site in which guidelines necessary in the daily work of a radiologist.
We invite you to take part in the formation of the section "To help the novice radiologist", determining the direction of its further development. We look forward to your feedback and wishes.
Study plan (description scheme) of a plain chest radiograph
- Image projection (front or rear direct, right or left side, front or rear oblique: 1st or 2nd).
- Special conditions of radiography (in the position of patients sitting or lying down due to the severity of their condition; with respiratory dynamic blurring of the image in patients who are unconscious, etc.).
- The condition of the soft tissues of the chest (volume, structure, the presence of foreign bodies or free gas after injuries, etc.).
- The state of the skeleton of the chest and shoulder girdle(position, shape, size and structure of the bones: ribs, sternum, visible cervical and thoracic vertebrae, clavicles, shoulder blades, heads humerus; state of ossification nuclei and growth zones in children and young people).
- Comparative evaluation lung fields (area, shape, transparency). If symptoms of pathology are detected (extensive or limited darkening or enlightenment, foci, round or annular shadow) detailed description their position, shape, size, shadow density, structure, contours.
- State lung pattern(distribution of elements, architectonics, caliber, character of contours).
- The state of the roots of the lungs (position, shape, size, structure, contours of the elements, the presence of additional formations).
- The state of the mediastinum (position, shape and width of it as a whole and the characteristics of individual organs).
- X-ray morphometry.
- Recommendations.
Study plan (description scheme) of bone radiographs
- Field of study.
- Image projection (direct, lateral, axial, tangential, special, additional or non-standard in a serious patient).
- Assessment of image quality (physical and technical characteristics: optical density, contrast, image sharpness; absence of artifacts and veils).
- The state of soft tissues (shape, volume, intensity and structure of the shadow, the presence of foreign bodies or free gas after injuries, etc.).
- The position of the bone (usual, displacement due to dislocation or subluxation).
- The size and shape of the bone (normal, shortening or lengthening, thickening due to working hypertrophy or hyperostosis, thinning due to congenital hypoplasia or acquired atrophy, curvature, swelling).
- External contours of the bone, taking into account anatomical features(even or uneven, clear or fuzzy).
- Cortical layer (normal, thinned or thickened due to hyperostosis or enostosis, continuous or intermittent due to destruction, osteolysis or fracture).
- Bone structure (normal, osteoporosis, osteosclerosis, destruction, osteonecrosis, sequestration, osteolysis, cystic restructuring, integrity violation).
- X-ray morphometry.
- X-ray (clinical and radiological) conclusion.
- Recommendations.
Study plan (description scheme) of radiographs of the joints
- Field of study.
- Image projection (direct, lateral, axial, special, additional or non-standard in a severe patient).
- Assessment of image quality (physical and technical characteristics: optical density, contrast, image sharpness; absence of artifacts and veils).
- Condition of soft tissues (shape, volume, shadow intensity, structure, presence of foreign bodies or gas after injuries, etc.).
- The state of the x-ray joint space (normal width, deformed, narrowed evenly or unevenly, expanded evenly or unevenly, darkened due to calcifications or the presence of effusion, contains additional formations: bone fragments, foreign bodies, bone or cartilage fragments - articular mice).
- Growth zones and ossification nuclei in young people (corresponding to age, position, shape and size).
- The size and shape of the articular ends (normal, thickening or atrophy, swelling, flattening, mushroom-shaped deformity, etc.).
- Congruence (correspondence to each other) of the articular cavity and articular head.
- The position of the articular ends (normal, displacement due to dislocation or subluxation, indicating the direction).
- The contours of the endplates of the epiphyses (continuous or intermittent, smooth or uneven, clear or fuzzy, thickened or thinned).
- The structure of the subchondral (subchondral layer) (normal, osteoporosis, osteosclerosis, destruction, sequestration, cystic restructuring).
- The bone structure of the epiphyses and metaphyses (normal, osteoporosis, osteosclerosis, destruction, osteonecrosis, sequestration, osteolysis, cystic restructuring, violation of integrity).
- Periosteal reaction (absent, present: linear or detached, fringed, stratified or "bulbous", spicules or needle-like, periosteal visor, mixed).
- X-ray morphometry.
- X-ray (clinical and radiological) conclusion.
- Recommendations.
Study plan (description scheme) of spinal radiographs
- Field of study.
- Image projection (direct, side, oblique, others).
- Assessment of image quality (physical and technical characteristics: optical density, contrast, image sharpness; absence of artifacts and veils).
- The state of soft tissues, especially para - and prevertebral (shape, volume, intensity and structure of the shadow).
- The severity of physiological (lordosis, kyphosis) and the presence of pathological (scoliosis, kyphosis) bends.
- Vertebral condition:
- bodies (position, shape, size, contours, structure, ossification nuclei in young people);
- arches (position, shape, size, contours, structure);
- processes (position, shape, size, contours, structure, ossification nuclei in young people).
- The state of the intervertebral joints (facet, uncovertebral; in thoracic region costovertebral and costotransverse).
- The state of the intervertebral discs (X-ray intervertebral spaces) (shape, height, shadow structure).
- The state of the spinal canal (shape and width).
- Condition of other visible parts of the skeleton.
- X-ray morphometry (with functional research, scoliosis, etc.).
- X-ray (clinical and radiological) conclusion.
- Recommendations.
Study plan (description scheme) of plain radiographs of the skull
- Image projection (over 20 general and special projections).
- Evaluation of the correct laying (according to the criteria for each projection).
- Assessment of image quality (physical and technical characteristics: optical density, contrast, image sharpness; absence of artifacts and veils).
- The shape and size of the skull as a whole.
- The ratio of the brain and facial regions.
- Condition of soft tissues in the area cerebral skull(shape, volume, intensity and structure of the shadow).
- The state of the cranial vault (shape and size; thickness and structure of the bones, the condition of the outer and inner plates and the spongy layer; the position and condition of the sutures; the condition of the vascular sulci, venous graduates, pachyon pits; the severity of "finger impressions"; pneumatization of the frontal sinuses).
- Condition of the base of the skull (configuration and dimensions; boundaries and contours of the anterior, middle and posterior cranial fossae; dimensions of the angles of the base of the skull; condition of the Turkish saddle; pneumatization of bones; condition of natural openings in the area of the base of the skull and pyramids temporal bones).
- The presence of calcifications in the skull and analysis of their shadow (physiological or pathogenic).
- general review facial department skulls (shape, size).
- The state of soft tissues in the region of the facial skull (shape, volume, intensity and structure of the shadow).
- The state of the eye sockets (shape, size, contours).
- Nasal cavity and pear-shaped opening (position, shape, size, pneumatization, condition of nasal conchas).
- The state of the cells of the ethmoid labyrinth (position, shape, size, contours, pneumatization).
- Condition of the maxillary sinuses (position, shape, size, contours, pneumatization).
- The condition of the visible sections of the jaws and teeth.
- X-ray morphometry.
- X-ray (clinical and radiological) conclusion.
- Recommendations.
Study plan (description scheme) of radiographs with contrasting of the organs of the urinary system
- The conditions of the study (type, concentration, amount and method of administration of a contrast agent; number, projection and sequence of images; position of the patient, respiratory tests, other conditions).
- Evaluation of the quality of the image (the quality of the patient's preparation for the study; physical and technical characteristics: optical density, contrast, image sharpness; no artifacts).
- The state of the visible parts of the skeleton.
- The condition of the surrounding soft tissues and neighboring organs.
- Contours of the psoas major muscles, compared on both sides (determined or not; even, uneven; clear, fuzzy).
- The position of the kidneys.
- Kidney shape.
- Kidney sizes.
- Contours of the kidneys.
- Intensity and structure of the shadow of the kidneys.
- The presence of additional shadows in the projection of the urinary tract and other organs of the retroperitoneal space and abdominal cavity suspicious for calculi, petrifications, tumors, etc.
- Comparative assessment of the release of a contrast agent by the kidneys (timing and severity of the nephrographic phase, timing and nature of the filling of cavity systems with contrast).
- The position, shape and size of the calyces and pelvis.
- Position, shape, contours and width of the lumen of the various parts of the ureters.
- The degree and nature of the filling of the ureters with a contrast agent.
- Position, shape, size Bladder.
- Contours and structure of the bladder shadow.
- X-ray morphometry.
- X-ray (clinical and radiological) conclusion.
- Recommendations.