Pain in the left side of the pelvis. Chronic pelvic pain syndrome in women: symptoms
Prevalence, causes, diagnostic search
Inna Wilhelmi
operating obstetrician-gynecologist of the Center of Urology and Gynecology of the ANO Clinic NIITO, Novosibirsk
Areas of interest: genital prolapse, urogynecology, aesthetic gynecology, laparoscopy, endometriosis
Every tenth patient who consults a gynecologist complains of chronic pain. The term “pelvic pain” refers to pain localized in the lower abdomen, lumbar region and sacrum, as well as in the perineum, external genitalia, vagina and rectum.
Usually this is a symptom of an underlying disease, but chronic pelvic pain syndrome (CPPS) itself is also distinguished. Currently, there is no uniform terminology, and increasingly, instead of the term CPPS, the term “chronic perineal-pelvic pain and dysfunction syndrome” is used, which better reflects the essence of this disease.
Definition
Chronic pelvic pain syndrome is a condition characterized by:
- nonspecific pelvic pain of uncertain onset, present for at least 6 months
- absence of changes in organs and tissues that can explain the severity of the pain syndrome
- significant reduction in quality of life.
About 15–30 % of all medical consultations are for pain symptoms that are not medically explained points of view . Often, thorough studies conducted by doctors of related specialties: gynecologist, urologist, proctologist, neurologist, show the absolute norm.
Epidemiology
IN Russian Federation There are no statistics on CPPS, and according to the International Chronic Pelvic Pain Association, the prevalence of CPPS among women visiting a gynecologist reaches 15 %. CPPS is the indication for up to 40 % of laparoscopies and 10–15 % of hysterectomies performed annually in the United States.
Pathogenesis
The pelvic organs are closely connected to each other, have a common afferent and efferent innervation, blood circulation, so damage to one organ often involves neighboring organs in the pathological process. However, initially, women with chronic pelvic pain syndrome turn primarily to gynecologists. Sometimes, after an incorrect diagnosis is made, surgery pelvic pain (hysterectomy, presacral neurectomy, dissection of the uterosacral ligaments), which leads to aggravation of the clinical picture.
A risk factor for chronic pain syndrome is previous ineffective treatment of the underlying disease. In case of untimely and insufficient relief of acute pain, the pain sensitivity threshold decreases, persistent generators of pathological impulses arise, and the nociceptive system is activated. Chronic pain loses its connection with damage to the pelvic organs and is maintained through complex central mechanisms, acquiring the status of a disease itself. Constant pain leads to the formation of psycho-emotional disorders, which, in turn, further stimulate the process of chronic pain syndrome.
Not all patients with predisposing factors develop chronic pelvic pain. What matters is a woman’s personality type, lifestyle characteristics, social status, level of intelligence, marital status, etc. Thus, single women with a low income, low social status, prone to depression, neuroses are typical patients at an appointment with a gynecologist, neurologist, urologist with complaints of pain of an unspecified nature.
In chronic pelvic pain syndrome, the autonomic nervous system plays a major role in conducting and intensifying pain impulses. Irritation of sensory receptors of the autonomic nervous system perceived as spilled painful sensation, unclear localization, with blurred boundaries.
Chronic pelvic pain syndrome in women: symptoms
Women suffering from pelvic pain typically have complaints such as:
- heaviness, discomfort, pain in the lower abdomen or lumbar region
- painful menstruation (dysmenorrhea)
- dyspareunia (pain during, immediately before, or after sexual intercourse)
- vulvodynia (burning or stabbing pain in the perineum and vestibule of the vagina)
The pain can be cyclical or constant. A connection with the menstrual cycle most likely indicates a gynecological pathology (often endometriosis or inflammatory diseases). Ovulatory pain regularly appears in the middle menstrual cycle, dysmenorrhea is sometimes so severe that it deprives a woman of her ability to work these days. However, due to the presence of viscero-visceral connections, the cyclic nature of pain does not always exclude pathology of neighboring organs.
Particular attention is paid to the patient’s lifestyle, social status, financial situation, obstetric history, surgical interventions, sexual disorders. With the prolonged existence of pelvic pain, women become irritable, sleep disturbances appear, performance decreases, and ultimately they lose interest in life, up to the development of depressive, hypochondriacal conditions, decreased quality of life and social maladjustment. Therefore, in case of pronounced affective symptoms of chronic pelvic pain, it is advisable to immediately schedule a consultation with a medical psychologist, psychiatrist or psychotherapist.
Diagnostics
There is no single algorithm for the examination and treatment of patients with CPPS. A diagnostic search always begins with a thorough collection of complaints and anamnesis of the disease and life.
According to the International Chronic Pelvic Pain Association, there are 6 obligate of this disease signs:
- duration of pain syndrome is at least 6 months
- low effectiveness of therapy
- discrepancy between the intensity of the patient's pain and the severity of tissue damage
- presence of signs of depressive disorder
- progressive limitation of physical activity
- presence of depression, hypochondria
The complex of basic examinations for CPPS includes:
- A thorough examination with bimanual vaginal and rectal examination, general clinical examination.
- Screening for STIs (especially herpes and chlamydial infections).
- Ultrasound of the pelvic organs, kidneys, bladder, abdominal cavity, including assessment of blood flow in the pelvic vessels with the Valsalva maneuver and with a change in body position; in some cases, MRI or MSCT of the pelvis is justified.
- X-ray examination of the lumbar sacral region spine, pelvic bones in two projections, irrigoscopy, urography, densitometry.
- Endoscopic examination methods: hysteroscopy, cystoscopy, fibrogastroscopy, colonoscopy.
- Consultation of related specialists: therapist, urologist, neurologist, surgeon, gastroenterologist, proctologist, psychologist.
- Diagnostic laparoscopy if less invasive diagnostic methods are unsuccessful.
Treatment of chronic pelvic pain
Treatment of chronic pelvic pain syndrome in women is a complex problem and is carried out based on the identified etiological factor. In addition, if the pain syndrome is severe, symptomatic therapy is necessary. The main goal of treatment is to improve the quality of life.
For symptomatic therapy, non-narcotic analgesics and physiotherapeutic methods of influencing the sources of pain impulses are most often used.
Despite the widespread use of analgesic drugs for the treatment of CPPS, in particular non-steroidal anti-inflammatory drugs, there are no reliable studies on their effectiveness.
Considering the pathogenesis of pain, an interdisciplinary approach is always most appropriate in the treatment of CPPS. In the Russian Federation there are currently no specialized centers for the study of chronic pain and very few specialists dealing with this problem. To provide effective assistance Such patients need the creation of specialized teams, which should include doctors of several specialties (gynecologists, urologists, neurologists, surgeons, gastroenterologists, proctologists, physiotherapists, rehabilitation specialists, psychologists, psychotherapists, sex therapists), armed not only with specific knowledge about the mechanisms of pain syndrome, but and modern equipment, including diagnostic, endoscopic, electrophysiological.
List of sources
- Giamberardino M. A. Women and visceral pain: are the reproductive organs the main protagonists? Mini-review at the occasion of the “European week against pain in women 2007”. Eur.
- J. Pain. 2008; 12 (3): 257–60.
- Vorobyova O.V. Chronic pelvic pain: focus on myofascial pain syndrome of the pelvic floor muscles. Consilium medicum. 2012: 6 (14): 14–8.
- Yarotskaya E. L., Adamyan L. V. Features of tactics for managing gynecological patients suffering from pelvic pain. Reproduction problems. 2003; 3: 17–26.
- Yarell J., Giamberardino M. A., Robert M., Nasr-Esfabani M. Bed-side testing for chronic pelvic pain: discriminating visceral from somatic pain. Pain Res. Treat. 2011; 11: 692–8.
- Chronic pelvic pain. ACOG American Congress of Obstetricians and Gynecologists. www.acog.org.
- Vulvodynia. ACOG American Congress of Obstetricians and Gynecologists. www.acog.org.
- Howard F. M. The role of laparoscopy in the chronic pelvic pain patient. Clin. Obstet. Gynecol. 2003; 46: 749–66.
- Missmer S. A., Cramer D. W. The epidemiology of endometriosis. Obstet. Gynecol. Clin. North Am. 2003; 30:1–19.
Make an appointmentFor your convenience, at the Energo clinic on the street. Kyiv, 5 is open. We offer expert consultations with gynecologists, urologists, and endocrinologists. The Center has modern equipment from leading global manufacturers. And most importantly, we take care of our patients, creating a calm, friendly atmosphere.
We will be happy to help you!
Pain and discomfort never appear just like that; it is always a sign of a disruption in the normal functioning of the body, which can be caused by a minor sprain/bruise or a serious illness. Pelvic pain syndrome in gynecology is a common occurrence, but patients do not always consult a doctor about it. The most common treatment option is to take painkillers and hope that it will “go away on its own.”
But the fact is that pelvic pain in women of reproductive age or menopause can be a signal of a gynecological and other disease, and if it is not treated, serious complications can arise.
Pelvic pain syndrome is:
- any painful and uncomfortable sensations in the lower abdomen or in the lumbosacral region;
- periodic or constant pain, and the pain can be sharp, dull, aching, or “give” to the rectum or vagina. This pain is not caused by pregnancy or menstrual syndrome, that is, it has other causes.
Accordingly, if you experience pain and discomfort periodically or do not go away for a long time, then do not delay your visit to the gynecologist. You can take care of your health at the Energo medical clinic, where high-level specialists work and there is high-quality diagnostic equipment.
Chronic pelvic pain syndrome in women: symptoms
Painful sensations and severe pain in the pelvic organs can be caused by painful menstruation (algomenorrhea) or ovulation. But if the pain is not cyclical and lasts for several months, appearing in the pelvis, lower back, abdomen (below the navel) and worsening the general physical and emotional condition, in this case doctors most often diagnose “chronic pelvic pain syndrome” in women, and this is manifested by symptoms such as:
- constant pain of varying nature and intensity (pulling, dull, etc.) for a long time;
- periodic manifestations of exacerbations for various reasons (hypothermia, overwork, stress, etc.);
- decreased sexual function up to complete absence sexual desire;
- insomnia, weakness, excitability, irritability, anxiety, depression, impaired ability to work, attention, memory loss and other psycho-emotional disorders.
Of course, the main symptom is pain and tenderness in the pelvic organs. Employees of the Energo clinic recommend not to wait until the disease progresses to acute form with serious complications, and promptly contact a specialist. Even a routine consultation and selection of a simple treatment regimen will be useful.
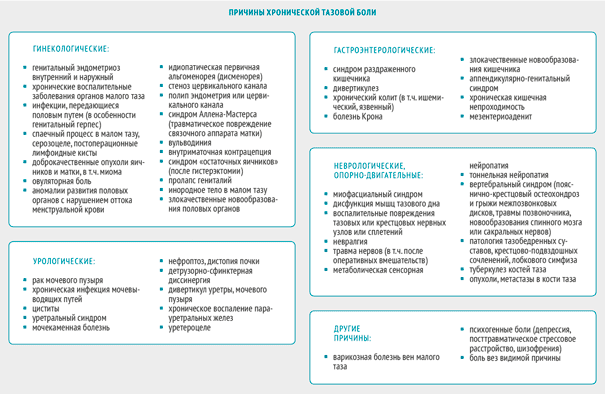
Chronic pelvic pain syndrome in women: causes
The main causes of pain can be gynecological and non-gynecological in nature, which can only be determined by specialists during a personal examination and with the help of diagnostic equipment.
Gynecological causes of pain in the pelvic area:

Non-gynecological signs of the syndrome:
- various pathologies of the musculoskeletal system (osteochondrosis, arthrosis, intervertebral hernia, tumors and metastases in the pelvic bones and spine, tuberculous lesions of the musculoskeletal system, etc.);
- various pathologies gastrointestinal tract(proctitis, chronic colitis, appendicular-genital syndrome and irritable bowel syndrome, adhesive diseases, etc.);
- various diseases urinary system (urolithiasis, developmental anomalies internal organs, for example kidneys, incorrect location organs, nephroptosis of any degree, chronic cystitis, etc.);
- diseases of the peripheral nervous system (inflammation and damage to the nerve nodes of the pelvis or sacrum);
- various neoplasms of the retroperitoneal space, etc.
The situation is usually worsened by decreased immunity, stressful situations and self-medication. Do not endure pain and do not lead the syndrome to complications and longer and more expensive treatment - make an appointment with a doctor. You can find out the work schedule of specialists in the gynecological department of the Energo Medical Center, as well as make an appointment by calling the phone number listed on the page.
Initial inspection:
An initial examination by a specialist is the right step towards getting rid of painful sensations and prevent their reappearance, as well as the development of any complications.
Since the symptoms and causes of this disease are varied, an initial examination is needed to identify obvious problems, exclude any signs and causes, and also receive directions and recommendations for examination. Each case of chronic pelvic pain syndrome in women is always individual, and therefore treatment is prescribed according to a strictly individual plan.
At the initial appointment and examination, the doctor will ask a number of leading questions in order to obtain more information necessary for treatment (analysis of complaints and their nature, as well as medical history), and may also take a smear for analysis.
Diagnosis of the disease:
Primary diagnosis includes questions from the doctor about the following indicators:
- nature, duration, frequency and localization of pain;
- possible factors provoking the occurrence of pain;
- the work of other organs that may also be associated with pelvic pain;
- previous diseases, surgeries and sexually transmitted infections, etc.
A general gynecological examination will allow you to exclude obvious pathologies of the pelvic area and establish the localization of pain. It is possible to prescribe additional examinations in particularly complex cases.
Additional examinations
- exclusion tests infectious diseases(cytological examination of smear and scraping, ultrasound of the pelvic organs, magnetic resonance imaging);
- diagnostic laparoscopy to identify foci of endometriosis and adhesions;
- if related diseases are suspected, it is possible to schedule an examination with a neurologist, gastroenterologist, psychotherapist, mammologist and other specialists.
At the Energo Medical Center in St. Petersburg, the diagnosis of pelvic pain in women is carried out using modern equipment under the supervision of high-level specialists. The key to successful treatment is high-quality diagnosis and selection of the necessary medications, as well as restorative therapy.
Contraindications
Contraindications include individual intolerance to treatment components, allergic reactions and individual characteristics of the patient. You should immediately inform your doctor about any contraindications you know of.
Treatment plan:
Treatment can be carried out using:
- surgical intervention;
- manual therapy;
- reflexology;
- medicines.
Depending on the nature and type of chronic pelvic pain syndrome, medications for inflammation and infections, painkillers, antidepressants, etc. may be prescribed. A set of drugs and medicines is prescribed individually.
Repeated appointment and treatment control
A repeat appointment is necessary to assess the patient’s condition and how effective and useful the treatment is. If there is no progress in recovery, the doctor prescribes new examinations and tests in order to then formulate a new treatment plan.
Treatment result:
The timing and results of treatment and recovery are individual and are determined by the doctor after a complete diagnosis and examination of the patient. If one of the causes of pelvic pain is genital infections, then treatment is also prescribed for the partner.
Rehabilitation and physiotherapy
At the end of treatment, as a rule, a course of treatment is prescribed to restore the immune and other systems of the body: hormonal, enzyme and antioxidant therapy, vitamins and mineral complexes.
Prevention:
To prevent the development of this syndrome and its relapses, a good set of measures are physical activity and activity, protected sexual intercourse, increase and support immune system vitamins and mineral complexes, and proper nutrition and giving up bad habits.
But it is also better to get prescriptions for prevention from a specialist. To make an appointment with a specialist at the Energo Medical Center, use the online form on the website or call the phone number listed at the top right.
Shulpekova Yu.O.
The term " pelvic pain"came to domestic medicine from foreign medical publications; in them, pelvic pain is considered as a syndrome that serves as the basis for further differential diagnosis. However, it should be recognized that pain itself, without describing other signs stereotypically associated with it, is only a separate symptom.
“Pelvic” refers to pain localized in the lower abdomen below the navel, in the lower back and sacrum, as well as in the perineum, in the area of the external genitalia, vagina, and rectum. Irradiation along the anterior inner surface of the thighs and the lower edge of the buttocks is often observed. Typically, patients cannot indicate the exact localization of pain; it is rather diffuse in nature, and it is not always easy to separate the epicenter of pain from the zone of irradiation.
The temporal characteristics of pelvic pain - acute or chronic - are of fundamental importance for recognizing the causes and choosing treatment tactics.
Acute pelvic pain, usually sudden, severe, lasting up to several hours or days. Its causes are acute inflammatory diseases of the uterus and appendages, appendicitis, diverticulitis, acute colitis, acute urological diseases or conditions accompanied by ischemia of the pelvic organs or intraperitoneal bleeding - torsion or rupture of an ovarian cyst, ectopic pregnancy, complications of proctosigmoiditis. Acute pain is often accompanied by fever, reflex nausea, vomiting, signs of intestinal paresis, symptoms of general intoxication or internal bleeding. Patients with acute pelvic pain need immediate medical attention.
Chronic pelvic pain - recurrent or constant pain which has been bothering the patient for at least 6 months. The nature of the pain can be different: burning, cutting, stabbing, It's a dull pain, feeling of pressure or heaviness. The intensity of pain in the same patient can vary significantly.
This article will focus on chronic pelvic pain in women due to the particular relevance of this problem. The prevalence of chronic pelvic pain among women, according to National Institute US health reaches 15%. Other epidemiological studies are currently being conducted.
The studied causes of chronic pelvic pain in women combine various gynecological, urological diseases, as well as diseases of the intestines and musculoskeletal system. It is paradoxical that not all women suffering from these diseases develop chronic pelvic pain.
The question of the mechanism of pain chronization is urgent. In conditions of persistence pathological process, and sometimes in the absence of obvious organic pathology, chronic pain can be the result of a decrease in the threshold of perception when pain occurs under the influence of non-noxious stimuli. In such cases, pathophysiologists use the following terms:
hyperalgesia - the occurrence of pain when exposed to soft threshold stimuli;
allodynia - pain when exposed to physiological stimuli that normally do not have an irritating effect;
spontaneous painful spasms - pain that occurs generally in the absence of any influence on the sensory nerve endings.
The modern theory of pain explains the formation of chronic pain by dysfunction of the nerve pathways and centers that control the flow of pain impulses. In some cases, the main role is played by a decrease in the activity of the antinociceptive system, in others - the phenomenon of neuronal sensitization, in others - the development of neurogenic inflammation supported by constant nerve impulses and the production of substance P, a peptide encoded by the calcitonin gene related peptide (CGRP), and growth factor nerves and neurokinins in the affected organ.
Surgical interventions on the pelvic organs and rheumatic diseases predispose to the formation of chronic pain.
In maintaining painful sensations, great importance is attached to the phenomenon of hyperesthesia/hyperalgesia of soft tissues, manifested, in particular, by the formation of trigger points in the muscles and fascia of the pelvic floor. This phenomenon was first described by the English neurologist H. Head and the outstanding Russian clinician G.A. Zakharyin. Zakharyin-Ged zones, as a rule, correspond to certain dermatomes, at the level of which sensitive innervation of the affected organ and the corresponding area of soft tissue is provided.
Pelvic muscle soreness often accompanies urological diseases, and physical therapy for myofascial pain often cures chronic pelvic pain.
Chronic pelvic pain is characterized by irradiation, which manifests itself as a feeling of pain, burning or itching in more distant areas simultaneously with the appearance of pain impulses from the affected organ. This phenomenon is, in fact, close to the phenomenon of hyperalgesia of the corresponding dermatome.
A number of researchers also point to the existence of visceral hyperalgesia - mutual strengthening of pain impulses due to partial intersection of the innervation paths of two affected organs. It has been shown, for example, that women with inflammatory diseases of the genitals are more likely to suffer from attacks of renal colic; in the same group of patients, pain in the back muscles is often observed at the ThX-LI level. .
The threshold for pain perception may be reduced under the influence of negative affective and social factors. Women suffering from chronic pelvic pain (usually in the form of dysmenorrhea, dysparenuria and vulvodynia) are more likely to have a history of physical or sexual abuse and show signs of post-traumatic stress disorder. Such patients are more prone to depression.
Due to the variety of causes of chronic pelvic pain, a multidisciplinary research group has been created in the United States based on large medical centers carrying out registration and thorough analysis of the causes of each case.
Grade accompanying symptoms can be of great help in identifying the cause. Chronic pelvic pain rarely exists as an isolated symptom and is often combined with other complaints; it may be associated with defecation, urination, the menstrual cycle, and sexual intercourse.
The most important diagnostic value has the identification of obvious signs indicating, for example, damage to the excretory system (hematuria, dysuria, etc.), genital organs (pathological discharge, menstrual irregularities, infertility, rash herpetiformis, papillomatosis, etc.) or intestines (diarrhea, constipation , pathological impurities in feces, etc.). But in many cases, the symptoms are nonspecific, which makes diagnosis difficult.
For women suffering from pelvic pain, the following complaints are quite “universal”: pain localized in the abdomen or lower back, very painful menstruation, dysparenuria (pain during sexual intercourse, as well as immediately before or after it), vulvodynia (burning or stabbing pain). pain in the perineum and vaginal opening).
In men, the nature of the complaints is somewhat different: the localization of pain in the lower back, difficult or painful urination, pain or discomfort at the base of the penis, around the anus, in the scrotum, pain during ejaculation, and blood in the seminal fluid are more typical. Often these symptoms are unreasonably interpreted as manifestations infectious prostatitis.
There is often an “overlap” of symptoms, when the same complaints are noted in different pathological conditions. This is especially true for dysparenuria and vulvodynia.
For the purpose of differential diagnosis of chronic pelvic pain, it is important to establish whether it is cyclic (periodic) in nature. A connection with the menstrual cycle most likely indicates a gynecological pathology, in particular endometriosis or venous congestion in the pelvic cavity. "Algodismenorrhea (syn. dysmenorrhea)" - pelvic pain during menstruation. “Ovulatory pain” is observed in the middle of the menstrual cycle, is associated with ovulation and occurs quite regularly in some women; pain may persist for up to 2-3 days, relieved by the use of heat or analgesics.
And yet, the cyclical nature of the pain does not allow us to completely exclude the pathology of neighboring organs that are not related to reproductive system, since the existence of viscero-visceral reflexes is possible.
From the point of view of some specialists, true chronic pelvic pain should mean only cases of non-cyclical pain of unknown origin, when all known organic causes have been excluded. This rigorous approach helps to identify a group of patients with functional pain, often associated with mental disorders- by analogy with functional abdominal pain, characterized in the Rome III criteria. It must be noted that the diagnosis of “functional pelvic pain” has not yet been reflected in the Rome criteria.
Some symptom complexes observed in certain pathological conditions are described below.
Chronic pelvic pain due to pathology of the urinary system is most typical for disorders such as interstitial cystitis, bladder stones and tumors, and obstructive uropathy. Symptoms can be very different:
pain (a feeling of discomfort, a feeling of pressure) in the suprapubic region, intensifying as the bladder fills or after it is emptied.
pain in the suprapubic region, urethra during urination;
vaguely localized pain in the pelvic area, with possible irradiation;
imperative calls to urinate and/or frequent urination;
the presence of pathological impurities in the urine;
dysparenuria.
Of particular interest is a disease such as interstitial cystitis (“irritated, or painful, bladder"). This is a fairly common disease, the causes of which are not well understood. Approximately 90% of patients suffering from this disease are women; worsening symptoms are observed during menstruation or after sexual intercourse. Pelvic pain with interstitial cystitis is often combined with fibromyalgia syndrome chronic fatigue, irritable bowel syndrome, which indicates the common pathogenetic mechanisms of pain formation.
Chronic pelvic pain in gynecological pathology is characterized by a particularly frequent combination with dysparenuria, vulvodynia, and sometimes with dysuria and is often cyclical in nature. About 15% of visits to a gynecologist are due to chronic pelvic pain. Among the most common reasons pain is caused by endometriosis, inflammation and venous congestion in the pelvis.
Chronic pelvic pain due to inflammation of the pubic symphysis (osteitis pubis) is localized in the pubic area and intensifies when performing physical activity, when squeezing your hips, climbing stairs, or squatting.
Chronic pelvic pain with damage to the sensory nerves of the lower abdominal wall and pelvic area - n. Pudendus, n. ilio-inguinale, n. ilio-hypogastrum, n. genito-femoralis. Damage to these nerves can occur during childbirth, surgery, or systemic neuropathy. It is possible that in some cases neuropathy is caused by herpetiform viruses. The following symptoms may occur alone or in combination:
dysparenuria;
pain when urinating or defecating;
pain when sitting;
pain in the lower abdomen or back - constant or associated with changes in body position;
pain in the genitals (vulvodynia) radiating along the posterior inner surface of the thighs and buttocks.
Chronic pelvic pain in diseases of the rectum. Chronic proctalgia is one of the most common types of pelvic pain. Its causes can be injuries, cracks in the mucous membrane of the rectum and skin around the anus, stercoral ulcers, hemorrhoids, rectal prolapse, recurrent herpetic and cytomegalovirus infections, human papillomavirus infection, tumor, chronic pararectal abscess. Proctalgia is a striking symptom of functional anorectal disorders: musculus levator ani syndrome or nonspecific functional anorectal pain, proctalgia fugax.
Proctalgia can be observed as part of ischemic colitis, stercoral, ulcerative colitis, irritable bowel syndrome. Pain may be associated with sexual intercourse, bowel movements and passing gas; You should pay attention to pathological impurities in the stool, changes in the perianal area.
Chronic pelvic pain background inflammatory diseases intestines is characterized by a combination with tenesmus, diarrhea mixed with blood, mucus and pus, general weakness, and weight loss. Similar symptoms can be observed with ischemic colitis, which is also characterized by persistent flatulence, abdominal pain, and unstable stool.
Irritable bowel syndrome (IBS) is one of the most common causes of chronic pelvic pain in patients of both sexes. In typical cases, the pain is localized in the lower abdomen, mainly on the left, is spastic in nature and is combined with diarrhea, constipation, and bloating. The pain is worse after eating and relieved after defecation. According to the Roman criteria functional disorders with IBS, periods of pain must necessarily be combined with changes in stool frequency and stool consistency. IBS is also characterized by a feeling of “obstruction” in the rectum when straining during bowel movements, a feeling incomplete emptying rectum, mucus discharge with feces.
When IBS is combined with proctalgia, there is severe stabbing pain in the rectum during bowel movements and the passage of gas.
Exacerbation of symptoms is observed against the background of stress, anxiety or depression.
Along with pelvic pain in IBS, a whole range of other symptoms can be observed: dysparenuria, algodismenorrhea, dysuric disorders. It is also very typical to have signs of autonomic dysfunction accompanying migraine and anxiety and depressive disorders.
The literature indicates a close relationship between the two most common types of pain in women - pelvic pain and migraine. According to a study by the US National Institutes of Health, chronic pelvic pain occurs in 15-24% of women of reproductive age, and migraine occurs in approximately 20%. There is an “overlap” of these conditions: no less than 67% of women with chronic pelvic pain have migraine. One possible explanation for this is the peculiarities of the metabolism of prostaglandins or serotonin and the regulation of smooth muscle cell tone, another is the peculiarities of pain perception in such patients.
Myofascial pelvic pain syndrome is a disorder in which painful “trigger” points form in the pelvic floor muscles. The pain is aching or burning in nature, its localization is varied. On palpation, the muscles of the pelvic floor and pelvic girdle appear tense, and points of sharp pain are identified in them. This is often accompanied increased sensitivity or itchy skin that makes it difficult to wear clothes. Compression of sensory nerves by muscles also leads to itching and burning. Concomitant dysuric disorders, urgency, constipation, pain during defecation, and dysparenuria are often observed. Probably, myofascial syndrome is formed secondary to traumatic physical activity, joint diseases, frequent straining during bowel movements, repeated genitourinary infections as a consequence of injuries and childbirth - and makes a significant contribution to the persistence of pain. Analysis of medical records showed that patients with diagnoses of “vulvodynia”, “interstitial cystitis”, “chronic pelvic pain”, “non-bacterial prostatitis”, “neuralgia”, “IBS” often have signs of myofascial pelvic syndrome.
Dangerous symptoms, indicating the likelihood dangerous complications in patients with pelvic pain: intense or increasing pain, fever (>38.5°C) with chills, vomiting with blood, bleeding from the vagina or rectum, signs of blood loss, difficult or painful urination, increasing increase in abdominal size.
Diagnostic search. Because chronic pelvic pain and its associated symptoms can occur in different combinations and severity, diagnosis is often difficult. Sometimes the cause of pain remains unrecognized.
Analysis of complaints and medical history involves a thorough assessment of the nature and localization of pain (lumbosacral region, coccyx region, sacroiliac joint, pelvic floor, groin area, abdominal wall), duration and frequency, and the influence of provoking factors. It is necessary to clarify complaints from all organs and systems, and analyze in detail the gynecological and drug history.
Particular attention should be paid to the description of the first episode of pain, which may serve as a key to identifying the “generator” of pain.
Rectal and vaginal examination are mandatory components of the examination of a patient with chronic pelvic pain. It allows you to identify diseases of the genital organs, rectum, changes in perirectal tissue and “trigger” points of the pelvic floor.
According to experts, a medical examination, supplemented by an ultrasound examination of the pelvic organs, in most cases makes it possible to recognize the gynecological pathology that is the cause of pain. Experience shows that to establish pathology in the intestines or urinary tract It is often necessary to perform endoscopy with biopsy, irrigoscopy, urography, computed tomography or magnetic resonance imaging.
In difficult cases, the question of diagnostic laparoscopy is raised. Only with the help of this study can we reliably confirm the diagnosis of peritoneal endometriosis, adhesive disease and simultaneously carry out surgical treatment.
Effective treatment, of course, depends on a correctly established underlying diagnosis. Due to the wide variety of causes of pelvic pain, the author is not able to discuss in detail the treatment of each disease.
For cyclical pain, usually associated with premenstrual syndrome, menstruation or ovulation, the use of combined hormonal contraceptives or progesterone drugs. For dysmenorrhea, symptomatic medications are prescribed - analgesics and antispasmodics. Appropriate treatment for genital infections is provided. For example, the use of acyclovir or valacyclovir for herpes infection and the prevention of relapses of candidiasis can lengthen periods of remission and alleviate the manifestations of vulvodynia and dysparenuria.
In some cases, physiotherapeutic treatment is effective, physiotherapy, acupuncture, especially when the causes of pain are associated with nerve damage, birth injuries, and impaired tone of the pelvic floor muscles. An open pilot study evaluated the performance of a special device for identifying and neutralizing internal myofascial “trigger” points in patients suffering from urological diseases. The device applies dosed compression to the site of pain based on the indicators of the built-in algometer. For confirmed myofascial syndrome, muscle relaxants and blockade of “trigger” points can be used.
The use of tricyclic antidepressants and selective serotonin reuptake inhibitors not only eliminates depressive disorders, but also effectively supports the function of the antinociceptive system. Antidepressants are used in an individual dose, starting with a small one.
Surgical methods of treatment. If foci of endometriosis are detected on the peritoneum during diagnostic laparoscopy, they are ablated. Laparoscopic uterosacral nerve ablation and presacral neurectomy can be used to treat pelvic pain and unexplained dysparenuria, but these procedures are technically difficult and carry an increased risk of bleeding.
American researchers analyzed the experience of performing hysterectomy in patients suffering from endometriosis or chronic pelvic pain of unspecified origin, refractory to other treatment methods. In a large proportion of cases, after surgery, the quality of life of women improves, and the manifestations of dysparenuria decrease. But in 21-40% of women after a hysterectomy, pelvic pain persists, and in 5% it occurs for the first time. The chances of pain relief are lower if there is underlying depression.
Antispasmodics have an analgesic effect in situations where pain is caused by spasm or stretching of a hollow organ (in particular the intestine) or inflammatory process, accompanied by reactive spasm of smooth muscles and blood flow disturbances. Therefore, drugs of this class are very often used in the treatment of chronic pelvic pain.
Antispasmodics are perhaps an integral component of the treatment of patients with IBS, regardless of its severity. Taking into account the laws of chronic pain, the prescription of antispasmodics should be resorted to already at the earliest early stages illness in order to prevent the long-term existence of a flow of pain impulses from the affected organ. From this point of view, it is necessary to choose the safest and most effective antispasmodic that has high selectivity and power of action specifically on the smooth muscle cells of the pelvic cavity organs - the intestines, urinary tract, genitals.
Drotaverine hydrochloride (Ho-spa® manufactured by Sanofi-Aventis) is a selective inhibitor of phosphodiesterase (PDE) type IV, which controls the contractile activity of smooth muscle cells of the gastrointestinal tract and genitourinary system. Inhibition of type IV PDE is accompanied by an increase in the intracellular concentration of cAMP and disruption of the interaction between actin and myosin. Drotaverine also prevents the entry of calcium into smooth muscle cells and reduces the activity of calmodulin, a catalyst for muscle contraction. Since type IV PDE is actively involved in the development of inflammation, its inhibition is accompanied by an anti-edematous and anti-inflammatory effect. The high selectivity of the action of drotaverine compared to papaverine minimizes the likelihood of affecting blood vessels and myocardium. Drotaverine hydrochloride has no anticholinergic effects, which allows it to be prescribed without significant concerns. medicine both elderly patients and children.
The effectiveness of taking drotaverine hydrochloride (No-shpy®) at a dose of 80 mg 3 times a day. within 4-8 weeks. in the treatment of pain in IBS and its safety has been proven in randomized, double-blind, placebo-controlled studies involving 132 patients. The pronounced antispasmodic and analgesic effect of drotaverine is well known and confirmed in a number of studies. urolithiasis and gynecological pathology (painful menstruation, ovulatory pain, inflammatory diseases).
A multicenter, open-label, prospective study of the safety and effectiveness of drotaverine hydrochloride tablets (No-shpa®) in the treatment of irritable bowel syndrome was conducted in China. The study involved 217 patients aged 18-70 years, 52% were women. Patients are divided into four subgroups: IBS with a predominance of diarrhea, constipation, mixed course or nonspecific type. The group of patients with IBS with a predominance of diarrhea was the largest and included 45.6% of participants. All patients were prescribed No-shpa® 80 mg 2 times a day. within 2 weeks. The primary endpoint was the severity of abdominal pain (on a 3-point scale, where 0 points corresponded to the absence of pain), and the secondary endpoint was changes in the frequency, shape of stool, and associated symptoms. After two weeks of treatment, the severity of pain decreased significantly in all subgroups of patients; average in general group- from 1.42±0.42 to 0.66±0.59 points (p<0,0001). Результат действия в отношении облегчения боли в конце 2-й нед. лечения оценили как отличный - от 28 до 36%, как хороший - от 26 до 36% больных в разных подгруппах. Об отсутствии эффекта сообщили от 15 до 31% больных. По сравнению с концом 1-й нед. к концу 2-й нед. лечения число больных, отметивших существенное облегчение ("клиническое излечение"), увеличилось примерно вдвое. Дротаверина гидрохлорид оказывал положительное влияние на частоту и консистенцию стула. При CРК с преобладанием диареи средняя частота дефекаций в сутки уменьшилась с 2,8±1,2 до 1,6±0,8 (p<0,0001); при СРК с запором - увеличилась с 0,6±0,4 до 0,8±0,3 (р=0,0004). Последнее можно объяснить уменьшением спастической активности толстой кишки. Значительно уменьшилось число больных, испытывавших чувство затрудненной дефекации, неполного опорожнения прямой кишки, императивных позывов. Серьезных нежелательных явлений в ходе лечения не зафиксировано .
A pharmacoeconomic analysis of the use of antispasmodics for pain relief in IBS, published by A.V. Afonin, O.M. Drapkina, A.S. Kolbin, M.V. Pchelintsev, V.T. Ivashkin, showed that “drotaverine has faster dynamics in reducing the signs of spasm and associated abdominal pain in comparison with mebeverine and hyoscine butyl bromide, No-spa has clear clinical and economic advantages in terms of pharmacoeconomic parameters “cost-effectiveness” and “cost minimization”.
In recent years, much attention has been devoted to the problem of magnesium deficiency in the pathogenesis of reproductive diseases in women, as well as emotional disorders and increased neuromuscular excitability. The effects that magnesium has in the body are closely related to the action of pyridoxine (vitamin B6). These substances, acting synergistically, regulate the functions of many enzymes, prevent the accumulation of homocysteine and prevent thrombophilia. Magnesium is involved in maintaining the transmembrane potential and also reduces the production of thromboxane, exhibiting anti-inflammatory and antiplatelet effects.
In the modern diet of Russians, the magnesium content often does not correspond to physiological needs. The causes of iatrogenic magnesium deficiency can be the prescription of diuretics, cyclosporine, cardiac glycosides, antibiotics (especially aminoglycosides), adrenergic blockers, caffeine, theobromine, theophylline, anti-tuberculosis drugs, estrogen-containing contraceptives. Magnesium loss occurs with diarrhea. Under conditions of vitamin B6 and magnesium deficiency, pain sensitivity increases, probably partly due to impaired synthesis of neurotransmitters that regulate nociception - GABA, serotonin, dopamine.
With magnesium deficiency, pregnant women experience pelvic pain associated with impaired blood flow and tone of the uterus, as well as increased muscle excitability.
Organic magnesium salts (lactate, orotate, aspartate, citrate, pidolate) are absorbed significantly better than inorganic ones when taken orally. Combination with pyridoxine improves magnesium absorption. The combination of magnesium lactate 470 mg with vitamin B6 5 mg per tablet (MagneB6®) and magnesium citrate 618.34 mg with vitamin B6 10 mg per tablet (MagneB6 forte® produced by Sanofi-Aventis) can be used in the complex treatment of patients with chronic pelvic pain due to conditions accompanied by magnesium deficiency.
Literature
1. Afonin A.V., Drapkina O.M., Kolbin A.S., Pchelintsev M.V., Ivashkin V.T. Clinical and economic analysis of antispasmodics for the relief of abdominal pain caused by intestinal spasm. //Russian Medical Journal - Vol. 18, No. 13, 2010. - With. 845-9.
2. Baranskaya E. K. Abdominal pain: clinical approach to the patient and treatment algorithm. The place of antispasmodic therapy in the treatment of abdominal pain // Farmateka. - 2005. - No. 14.
3. Ivashkin V. T., Shulpekova Yu. O. Nervous mechanisms of pain sensitivity // Russian Journal of Gastroenterology, Hepatology, Coloproctology. - 2002. - No. 4. - P. 16-21.
4. Website http://www.aids.about.com/od/otherconditions/a/rectal_pain_2.htm - June 20, 2011
5. Website http://www.bettermedicine.com/article/pelvic-pain- June 20, 2011
6. Website http://www.cjge-manuscriptcentral.com/Web/ViewAbstract.aspx?GaoHao=wcbx 10000241 - July 12, 2011
7. Website http//www. clinicaltrials.gov - July 1, 2011
8. Website http://www.medikforum.ru/news/medicine_news/5148-tazovaya-bol-oznachaet-migren.html - June 20, 2011
9. Website http://painconsortium.nih.gov/MAPPResearch.html - July 2, 2011
10. Website http://www.romecriteria.org - July 1, 2011
11. Website http://www.sirweb.org/patients/chronic-pelvic-pain - June 20, 2011
12. Pchelintsev M.V. Antispasmodics: from clinical pharmacology to pharmacotherapy // Attending physician - No. 7, 2008. - With. 3-6.
13. Anderson R, Wise D, Sawyer T, Nathanson BH. Safety and Effectiveness of an Internal Pelvic Myofascial Trigger Point Wand for Urologic Chronic Pelvic Pain Syndrome. Clin J Pain. 2011 May 25.
14. Apte G, Nelson P, Brismee JM et al. Chronic Female Pelvic Pain-Part 1: Clinical Pathoanatomy and Examination of the Pelvic Region. Pain Pract. 2011 May 26. doi: 10.1111/j.1533-2500.2011.00465.x.
15. Chang L. Brain responses to visceral and somatic stimuli in irritable bowel syndrome: a central nervous system disorder? // Gastroenterol Clin North Am. - 2005, June; 34 (2): 271-279.
16. Check JH. Chronic pelvic pain syndromes--traditional and novel therapies: part I surgical therapy. Clin Exp Obstet Gynecol. 2011;38(1):10-3.
17. Chronic pelvic pain. ACOG American Congress of Obstetricians and Gynecologists. Website http://www.acog.org/publications/patient_education/bp099.cfm. Accessed May 18, 2011 - June 20, 2011
18. Cicchiello LA, Hamper UM, Scoutt LM. Ultrasound evaluation of gynecologic causes of pelvic pain. Obstet Gynecol Clin North Am. 2011 Mar;38(1):85-114.
19. Driul L, Bertozzi S, Londero AP et al. Risk factors for chronic pelvic pain in a cohort of primipara and secondipara at one year after delivery: association of chronic pelvic pain with autoimmune pathologies. Minerva Ginecol. 2011 Apr;63(2):181-7.
20. El-Din Shawki H. The efficacy of laparoscopic uterosacral nerve ablation (LUNA) in the treatment of unexplained chronic pelvic pain: a randomized controlled trial. Gynecol Surg. 2011 Feb;8(1):31-39.
21. Fitzgerald CM, Neville CE, Mallinson T et al. Pelvic floor muscle examination in female chronic pelvic pain. J Reprod Med. 2011 Mar-Apr;56(3-4):117-22.
22. Glasgow R., Mulvihil S. Abdominal pain, including the acute abdomen. Sleisenger&Fordtrans’s Gastroentestinal and Liver Disease. Philadelphia - London - Toronto - Montreal - Sydney - Tokyo, 2003; 1: 80-90.
23. Jacques E. Common Chronic Pelvic Pain Symptoms by Diagnosis Website http://www.pain.about.com/od/typesofchronicpain/a/CPP symptoms.htm.
24. Lamvu G. Role of hysterectomy in the treatment of chronic pelvic pain. Obstet Gynecol. 2011 May;117(5):1175-8.
25. Mayer E., Berman S., Suyenobu B. et al. Differences in brain responses to visceral pain between patients with irritable bowel syndrome and ulcerative colitis // Pain. - 2005, June; 115(3):398-409.
26. Meltzer-Brody S, Leserman J. Psychiatric Comorbidity in Women with Chronic Pelvic Pain. CNS Spectr. 2011 Feb 1. pii: Meltzer-Brody.
27. Misra SC, Pandey RM. Efficacy of drotaverine in irritable bowel syndrome: a double-blind, randomized, placebo-controlled clinical trial. Am J Gastroenterology 2000; 95: 2544 (Abs 455).
28. Musial F., Huser W., Langhorst J. et al. Psychophysiology of visceral pain in IBS and health // J. Psychosom. Res. - 2008, June; 64 (6): 589-597.
29. Neslihan Zehra Gultasl, Aydn Kurt, Ali Ipek, Mehmet Gumus, Kemal Rdvan Yazcoglu, Gulcin Dilmen, Ismet Tas The relation between pelvic varicose veins, chronic pelvic pain and lower extremity venous insufficiency in women. Diagn Interv Radiol 2006; 12:34-38.
30. Pap A, Hamvas J, Filiczky I, Burai M. Beneficial effect of drotaverine in irritable bowel syndrome. Gastroenterology 1998; 114: G3359 (AGA Abs).
31. Prendergast S. Myofascial pelvic pain syndrome Website http://www.examiner.com/pelvic-health-in-national/myofascial-pelvic-pain-syndrome - June 20, 2011
32. Soleymani H, Ismail L, Currie I. GPs should be vigilant for pelvic inflammatory disease. Practitioner. 2011 Mar;255(1738):15-8.
33. Vulvodynia. ACOG American Congress of Obstetricians and Gynecologists. Website http://www.acog.org/publications/patient_education/bp127.cfm. Accessed May 18, 2011 - June 20, 2011
34. Warren JW, Morozov V, Howard FM. Could chronic pelvic pain be a functional somatic syndrome? Am J Obstet Gynecol. 2011 Apr 14.